

Welcome to the Scrambler Therapy® official scientific and clinical information site
Welcome to the Scrambler Therapy® official scientific and clinical information site
Scrambler Therapy success on neuropathic and oncologic pain is statistically very high but strictly dependent on correct usage and compliance with standard protocols described in this site and primary training courses. Apart from diseases that call for more experience (phantom limb, painful anesthesia, pudendal neuralgia, trigeminal neuralgia, and some specifically severe forms of CRPS or CIPN), the minimum success (pain relief > 50%) should overtake by far 80%.
A multicentric monitoring activity (in hospitals and independent university clinics) on a broad range of patients nonresponsive to other treatments confirmed that the correct treatment methodology and protocols allow for optimal success rates higher than 90%, and in cases of higher operator-dependent variables, generally higher than 80%. Whereas, where methods and standard protocols are only partially followed, success percentage drops progressively in a related way. Even if in treated diseases a 50% success rate where other treatments have failed can be clinically considered as a great success, it is clearly not so for patients who have not benefited from this success. Note that the monitoring outcome is in line with official scientific publications that present the same misalignment in success percentage rates clearly for the same reasons.
Scrambler Therapy was created in Italy, where it has been used in the hospitals since the '90s. Primary and advanced training is carried out in Italy, and Prof. Marineo broadly cooperates with an excellent hospital for the recovery of specifically complex and/or apparently nonresponsive treatment. Most of these severe cases come from abroad. In this Italian structure, highly qualified in ST usage, specifically “difficult” cases are often brought back to success conditions.
Since 2011, this recovery program has hosted patients from Italy and abroad who clearly presented higher than average difficulty in treatment, but also cases with no specific criticality. The reasons for the unsuccessful treatment of nonspecific critical cases have been analyzed. Here is a list of the common reasons that led to wrongly considering patients as nonresponsive.
Correct training is paramount for good clinical practice of the methodology. The issues that surfaced in this sector are usually:
- Arbitrary changes of the standard protocols and training methods.
- The trained staff is not the same one who carries out the treatments or does not have an adequate knowledge of neuropathic and oncologic pain.
- Commercially, in the US, “Calmare® Certified” treatment centers are certified based on quality criteria autonomously set by the former local distributor. Information gathered during the monitoring activity recorded that these criteria are relevantly not in line with the official ones, and we deem they do not guarantee ST quality standards. Apart from commercial certifications, a correct treatment is only the one that follows standard protocols and methodology indicated on this website and on the official scientific documents.
- In some cases, according to the patients' description, correct procedures are not followed or are carried out by operators who lack adequate training to fulfill the treatments.
- Patients are given wrong information on the therapy and the treatment's scientific and neurophysiological aspects. Assuming that this is done in good faith, it is, however, an indication of possible execution problems in a correct treatment cycle due to the clear lack of methodology knowledge and, more generally, of clinical and neurophysiological aspects connected to chronic pain.
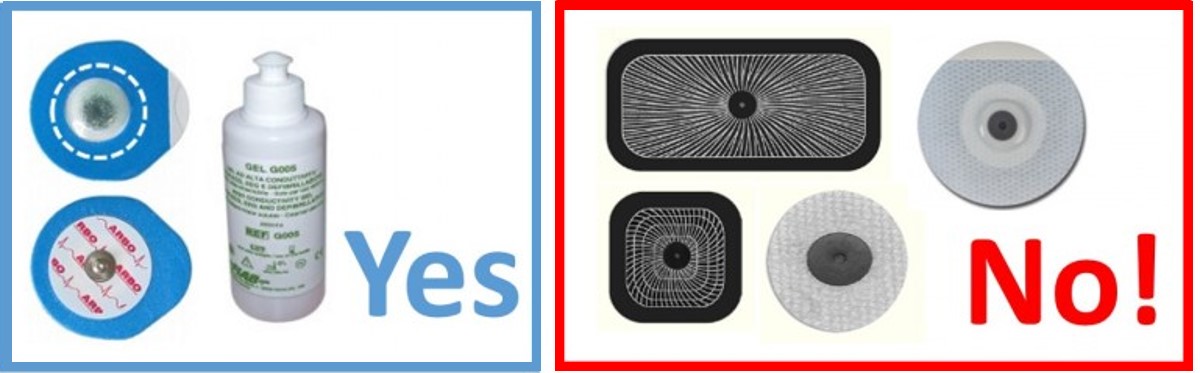
- Often electrodes different from the ones selected as optimal with spongy contact surfaces have been used. In these cases, distortion of information, which renders the patients' perception less comfortable, can determine a less effective treatment, and in the most critical cases, it prevents a successful stimulation fine-tuning.
- It is specifically wrong to use “large” electrodes like the ones usually used for TENS. In this case, apart from the problems previously listed, the broad electrode surface, because of its poorly selective recruitment, can stimulate wrong areas. This could lead to a pain increase during or after the treatment.
- Electrodes are reused, impairing the ability of ST to transmit information and prompting skin irritation.
- Gel is not added to optimize conduction.
- A normal treatment cycle consists of 10 treatments in a two-week timespan. This treatment cycle changes when:
1. The patient must be weaned off anticonvulsants for analgesic usage during the ST cycle. In this case one must consider the 10 treatments plus the ones needed for the weaning.
2. The pain is zero before the end of the 10 treatments. In this case the treatment cycle must end in advance. Important note: the treatment cycle must be considered effective only when the pain during the treatment is zero or not higher than 1/10. Zero pain must also include specific movements or positions. In this case the patient must be tested in the position or movement when he or she habitually starts to feel the pain before the stimulation. One must never exceed these limits, which will spontaneously progress throughout the treatment cycle. Once zero pain has been tested under this condition, the patient must return to an analgesic position for the remaining part of the treatment. The treatment can continue beyond the statistical limits only if:
3- The previous points have been followed
4- The patient continues to show clear signs of progressive improvement.
- Pain during stimulation is zeroed out or is not higher than 1/10. This condition must be true also in specific positions and movements that would normally evoke pain.
- During the treatment after stimulation fine tuning the patient must be in a most comfortable (analgesic) position.
- The patient can feel different sensations, but he/she must never feel a continuous “single sting” or “burning.” In general, the patient must never feel discomfort. The sole benchmark is absence of pain and no discomfort.
- A properly trained operator, when using more than one channel, will position them one at a time, checking the efficacy in the covered area (zero pain and no feeling of discomfort or a persistent single sting or burning). Once the positioning of the first channel has proven effective, the operator will follow the same procedure in positioning other electrodes (if necessary).
- During the treatment session, the patient might feel a progressive reduction in the stimulation intensity. The operator must increase the intensity to the optimal threshold perception.
- A center using STDM software is a clear sign of more care in abiding by correct standards of Scrambler Therapy usage.
- In general, one can find on this website further, more detailed information that allows one to better understand the treatment, such as:
10 basic rules to use Scrambler Therapy correctly
Adverse interactions and protocol adjustmen t
Pseudo chronic pain and
treatment expectations
Frequent errors
ST-NET usage in system-quality
for clinical trials and pilot centers
Contact Download Video Tutorial Delta Research & Development
Copyright © Delta Research & Development. All rights reserved